Nobody talks about this enough. Nurses and clinicians working in diverse communities across the UK deal with language barriers on a near-daily basis, yet the training most of us receive on how to actually handle it is minimal at best. You get a policy document. Maybe a module during induction. And then you’re on the ward, with a patient in front of you who speaks no English, and you’re figuring it out as you go.
That’s the reality. And it’s one worth being honest about.
This guide is aimed at nurses, student nurses, and clinicians who want a clear and practical understanding of language support in clinical settings. It draws on UK government guidance for migrant health, GMC standards, and NMC requirements. It’s also useful revision for anyone working through their CBT exam preparation, since questions around communication and patient safety come up regularly.
The focus throughout is on what actually works, what the rules are, and why cutting corners here tends to end badly.
The Real Cost of Getting This Wrong
Language barriers in healthcare are a patient safety issue. Not a communication inconvenience, not a diversity and inclusion talking point. A safety issue with real consequences.
When a patient doesn’t fully understand what a clinician is telling them, things go wrong in very predictable ways. Medications get taken incorrectly. Follow-up appointments get missed. Symptoms that should have been flagged don’t get mentioned because the patient didn’t have the words for it or didn’t understand the question. Consent gets given without genuine understanding of what’s being consented to.
The GMC is explicit about this. Clinicians have a duty to make all reasonable efforts to communicate effectively with their patients. That duty doesn’t disappear because a patient doesn’t speak English.
One scenario worth thinking about: a patient arrives in A&E with chest pain. They’re clearly uncomfortable, they’re gesturing at their chest, but beyond that communication is breaking down. Without an interpreter, the clinician might catch the headline complaint but miss the detail, pain radiating to the arm, breathlessness that started two hours ago, a family history the patient is trying to mention. These aren’t small details. In a cardiac presentation they can change the whole clinical picture.
Research on this is consistent. Professional interpreting reduces diagnostic errors, improves prescribing accuracy, and leads to better adherence to treatment plans. The evidence for using informal alternatives, such as family members or bilingual colleagues, points in the opposite direction.

Interpreting vs Translation: Worth Getting Clear On
These get used interchangeably all the time and it does cause confusion in practice.
Interpreting is spoken, real-time conversion of language. It’s what happens during a consultation when an interpreter is present or on the phone. Translation is written. It’s the process of converting a discharge letter, a consent form, or a patient information leaflet into another language.
Most clinical encounters require interpreting. And the type of interpreting matters too.
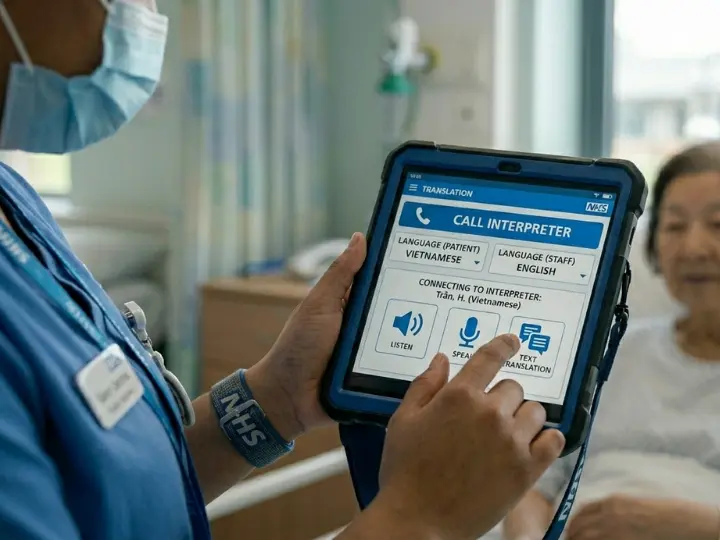
Face-to-face is the most effective option. A good interpreter in the room picks up on hesitation, distress, the way someone’s voice drops when they mention something they’re ashamed of. That non-verbal layer is clinically meaningful, especially in mental health consultations, safeguarding conversations, or when you’re breaking difficult news. You simply don’t get that over a phone call.
Telephone and video options do have their place though. They’re faster to arrange and much more cost-effective. For a routine follow-up or an urgent query where a face-to-face booking isn’t feasible, they work well. Just know that interpreted consultations run longer, typically around twice the usual duration, so build that into scheduling.
NHS providers are obligated to offer language support free of charge. Your trust will have a booking system. If you don’t know how to use it, find out before you need it in a hurry.
What to Actually Do When Your Patient Doesn’t Speak English
There’s a straight-forward protocol for this, and it’s worth knowing well enough that you don’t have to think hard about it in the moment.
Record language needs at first contact:
The patient’s preferred language and any dialect should go into their records straight away, not as an after-thought. This information needs to travel with them through every stage of their care, appointments, letters, phone calls, all of it.
Use your trust’s interpreter booking system:
Specify the language, the dialect if relevant, whether a same-gender interpreter is needed, and what topics the appointment will cover. If it’s a specialist area, brief the interpreter beforehand. Some clinical terminology doesn’t translate easily and an unprepared interpreter in an oncology consultation, for example, will struggle.
Allow enough time:
Double your usual slot. At the start, introduce the interpreter and make sure the patient understands who they are and what their role is.
Speak to your patient, not the interpreter:
This is the one people most commonly get wrong. Keep sentences short. Pause often. Check comprehension actively rather than accepting a nod as confirmation.
Document and carry it forward:
Note what language support was used and flag it in the patient record. Offer a written summary in the patient’s language where you can. The next clinician who sees this patient should already know what they need before they walk in the room.
For NMC CBT candidates:
If the question asks how you obtain information from a patient who doesn’t speak English, the answer is to use a face-to-face or online professional interpreter. Not a family member, not a bilingual colleague pulled off the ward. A professional interpreter. This maps directly to GMC duties and is the answer the exam is looking for.
Working with Interpreters Well
Booking an interpreter and using one well are two different things. Worth saying that clearly because the difference shows up in the quality of what you actually get from a session.
Preparation matters more than most people give it credit for. If the consultation involves complex or specialist content, share what you’ll be covering in advance. An interpreter who knows they’re about to sit in on a neurology review or a psychiatric assessment can prepare. One who walks in cold may not have the vocabulary they need.
During the session itself: look at the patient. They are your patient. The interpreter is there to facilitate the conversation, not to become the focus of it. Use diagrams, visual aids, medication cards where they help. For patients managing ongoing conditions especially, showing rather than just telling makes a real difference to how information lands.
Children must not interpret. Not for a quick question, not for anything. It puts an unfair burden on the child and it’s ethically indefensible. The same goes for pressuring family members into it because it’s convenient.
After a particularly difficult session, a brief debrief with the interpreter can be useful. And if you’re noticing a pattern where certain patient communities are consistently needing language support, that information is worth passing up the chain. It may be a case for more dedicated provision.

Why Family Members Cannot Be Your Interpreter
It’s understandable why this happens. A relative is right there, they speak the language, and arranging a professional interpreter takes time you may not feel you have. But using a family member as your interpreter is a practice that creates serious problems, and the NHS is clear that it should not be the default.
The issue isn’t just accuracy, though that’s a significant part of it. Family members often unconsciously filter what they relay. They leave out the parts that seem embarrassing or that they themselves don’t want to deal with. A daughter interpreting for her elderly mother may soften a mental health disclosure. A husband interpreting for his wife may not pass on details she’d share with a female clinician alone.
And then there’s confidentiality. Many patients will not say what they need to say in front of a family member. This is especially true for anything touching on mental health, sexual health, domestic situations, or social circumstances. You end up with an incomplete clinical picture and, more importantly, a patient who didn’t feel safe enough to tell you the truth.
Professional interpreters work to a strict code. Accuracy, impartiality, confidentiality. The outcome data when professional versus informal interpreting is compared is not ambiguous: professional services produce better care.
If you genuinely cannot access professional support in an emergency, the patient’s consent must be obtained independently and the arrangement must be clearly documented. It’s a last resort, not a workaround.

How This Plays out Across Different Settings
Mental Health
Migrants and refugees often carry trauma that is hard to articulate in any language. Being able to express psychological distress accurately, in your own words, matters enormously for getting the right assessment and diagnosis. Interpreters who work in mental health settings also understand the cultural dimensions of how distress gets expressed, something a family member interpreting for the first time simply won’t have the background to manage.
Maternity and Women’s Health
Cultural norms around pregnancy, reproductive health, and intimate examinations are deeply embedded for many communities. A same-gender interpreter is often not just a preference but a genuine prerequisite for the patient engaging with care at all. Women also need to understand their entitlements, including free GP registration during pregnancy, and that information has to reach them in a language they actually understand.
Long-term Condition Management
Diabetes, hypertension, asthma, COPD. Managing these conditions well depends on clear, repeated communication over time. A misunderstood medication change or a piece of lifestyle advice that didn’t land can lead to an avoidable exacerbation. Language preferences must be recorded and passed on so that continuity of care is real rather than just a phrase in a policy document.
Emergency and Acute Settings
Telephone interpreters can be brought in quickly and are good enough for initial triage. For anything more involved, taking a detailed history, obtaining informed consent, explaining a procedure or diagnosis, face-to-face interpretation is the safer option and should be arranged as soon as it’s practically possible.

The Systemic Angle: Health Equity
Language support isn’t only a clinical decision made at the bedside. It reflects something about how a health system is set up and who it’s actually designed to serve.
When language barriers are consistently unaddressed, the effects aren’t random. They fall on specific communities, typically those who are already more vulnerable, more likely to have gaps in their care history, less likely to push back when they don’t understand something. Over time that compounds into measurable health inequalities.
There’s also a cost argument that often gets overlooked. Interpreter services are not cheap, but a single avoidable emergency admission costs considerably more than months of interpreted outpatient appointments. The investment makes clinical and financial sense.
For training providers including Mentor Merlin’s OSCE and CBT preparation teams, embedding this understanding early is important. Nurses who understand why professional interpreting matters, not just what the policy says, are better equipped to advocate for it in practice settings where shortcuts are sometimes quietly normalised.
| Type | What Works Well | Limitations | Best Suited for |
| Face-to-Face | Captures tone, body language and emotional nuance. Builds trust with patients over complex | Requires advance planning. Can be harder to arrange at short notice | Sensitive conversations, constant, mental health, end-of-life, complex, history-talking |
| Telephone or video | Quick to access, available 24/7, cost-effective or routine appointments | No visual cues. Extended sessions can be tiring. Less suited to emotionally complex content | Urgent queries, routine reviews, situations where face-to-face isn’t available immeditely. |
| Family member or informal | Immediately available and familiar to the patient. | High risk of filtering, inaccuracy, and confindentiality breach. Ethically problematic in most scenarios. | Not recommended. Only as an absolute last resort with documented, independent patient consent. |

To Summarise
Language support in clinical practice isn’t optional and it isn’t a nice-to-have. It’s part of delivering safe, lawful, equitable care. The GMC is clear on this. The NMC is clear on this. And the evidence from patient outcomes is clear on this too.
The good news is that the process isn’t complicated once you know it. Find out how your trust books interpreters. Record language needs early and carry them through. Use professional services by default, not as a last resort. Speak to your patient, not through them.
For CBT candidates, get comfortable with this topic. It comes up. The correct answer will always involve a professional interpreter.
For those already in clinical practice: if you’re working in a setting where informal interpreting has become the norm, that’s worth pushing back on. Not because it’s a policy requirement, though it is, but because the patients on the receiving end of that shortcut deserve better.
Read our detailed blog – “Avoid These Common Pitfalls After the UK NMC CBT in 2026” – to ensure your journey stays on track.
Why Wait? Just Merlin It!
Free Consultation – Chat now with a Mentor.