Evaluation is 8 minutes handover station during NMC OSCE. Clear communication during evaluation handover provides appropriate care to the patient. During clinical handovers, patient deterioration, emergency escalation, or multidisciplinary teamwork, nurses must communicate information accurately and confidently. One of the most widely used communication frameworks in healthcare is SBAR format.
SBAR handover format helps nurses organise information into a structured format that reduces misunderstandings and improves clinical decision-making. In the NMC OSCE, effective use of SBAR format is not only assessed as a communication skill but also as a demonstration of professional accountability and safe nursing practice.
Many students struggle with clinical escalation because they either provide too much irrelevant information or miss critical details. A structured SBAR communication approach helps you stay focused, concise, and clinically effective.
This guide explains the four key components of effective evaluation using SBAR:
- Situation
- Background
- Assessment
- Recommendation

What Is SBAR format in NMC OSCE?
[SBAR] stands for:
- S – Situation
- B – Background
- A – Assessment
- R – Recommendation
It is a structured communication tool used by healthcare professionals to share important patient information clearly and efficiently.
The framework is commonly used during:
- Nurse-to-doctor escalation
- Shift handovers
- Emergency situations
- Patient deterioration reporting
- NMC OSCE handover station
According to patient safety studies, communication failures contribute to a significant percentage of adverse healthcare events. Structured communication tools like SBAR reduce those risks by ensuring all critical information is communicated safely.
Why SBAR Is Important in Nursing
Effective nursing communication supports:
- Faster clinical decisions
- Better teamwork
- Improved patient outcomes
- Reduced medication errors
- Early recognition of deterioration
- Safer escalation processes
For international nurses entering the UK healthcare system, understanding SBAR nursing handover is essential because it reflects NHS standards of professional practice.
Why SBAR Is Important in the NMC OSCE
In the NMC OSCE, examiners assess not only your clinical knowledge but also your ability to communicate safely and professionally.
Many OSCE scenarios require candidates to:
- Escalate patient deterioration
- Report abnormal observations
- Communicate with senior staff
- Handover patient information
- Recommend interventions
Using the SBAR format demonstrates:
- Clinical prioritisation
- Professional communication
- Patient safety awareness
- Organised thinking
Common OSCE Scenarios Using SBAR
Examiners specifically look for whether you:
- Introduce yourself properly
- Use concise information
- Include relevant assessment data
- Make safe recommendations
- Escalate and refer appropriately

The Four Key Components of Effective Evaluation Using SBAR
The strength of SBAR communication lies in its structure. Each component has a specific purpose in clinical evaluation and escalation.
Let’s examine each section in detail.
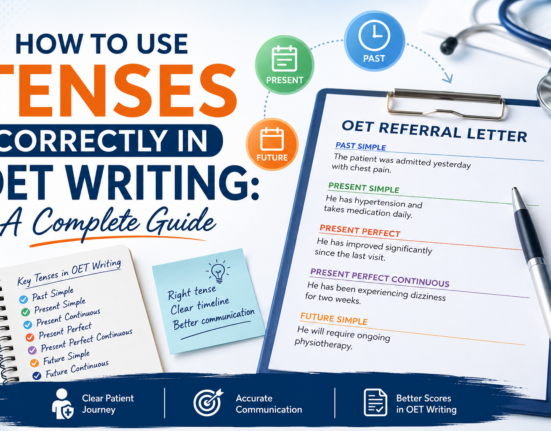
S – Situation
The [Situation] section explains the immediate issue that requires attention.
This is the most important opening because it quickly tells the healthcare professional:
- Who you are
- Where you are from (Department)
- Which patient you are discussing
- What the urgent concern is
The situation should be brief, direct, and clinically focused.
What to Include in Situation
You should include:
- Introduce yourself
- · The patient’s Name
- · Reason for admission
- · Patient date of birth, hospital number, date of admission or visit
- · Reason for handover
Example of Situation
Hi my name is Jenny; I am the registered nurse working in the surgical unit. I was looking after
Mr. John Smith who was admitted to the unit following his hernia repair. His hospital number
is 65034286 date of birth is 20.02.1970 and his date of admission is yesterday 8.00. I am here
to give you the handover as my shift ends now.
Why Situation Matters
An effective Situation statement:
- Grabs immediate attention
- Helps prioritise urgency
- Prevents delays in care
- Reduces confusion
In emergency settings, delays in identifying patient deterioration can significantly affect outcomes. A strong opening allows faster clinical responses.
Common Mistakes in Situation
Many nurses make errors such as:
- Giving too much irrelevant detail
- Speaking unclearly
- Forgetting patient identifiers
- Delaying the main concern
OSCE Tip for Situation
In the NMC OSCE:
- Speak calmly and confidently
- State the concern early
- Use professional terminology
- Prioritise patient safety
B – Background
The Background section provides important clinical context related to the patient’s condition.
What to Include in Background
Relevant details may include:
- History of patient admission (Diagnosis and Treatment)
- Allergic status and reaction
- Medical history from scenario
- Regular medications
- Most relevant information from social history
- Problem that can affect his activities of daily living
The information should directly relate to the current problem.
Example of Background
Mr. John smith was admitted with the complaints of pain and swelling on either
side of the pubic bone. After examination, he was diagnosed with inguinal hernia. John was
referred to the surgical team & they planned to conduct the surgery today. He is diabetic since
2017 and have hypertension since 2010, and is on Tab. Glucophage, 1gm and ramipril 5mg. He
partner has Alzheimer’s and earlier he said that his partner is taken by his daughter while he is
in the hospital, and he informed that daughter comes every other day and according to him she
will come to meet him tomorrow. An important point to be noted is, he is allergic to Penicillin
and the reaction is skin rashes
Why Background Matters
Good Background communication:
- Helps identify risk factors
- Improves treatment planning
- Prevents repeated questioning
- Enhances continuity of care

Choosing Relevant Information
One of the biggest communication challenges is deciding what information is relevant.
Include:
- Information directly linked to scenario details
- Clinical risk factors
- Important medications
Common Background Mistakes
Errors include:
- Providing too much information
- Missing important risk factors
- Forgetting allergies
OSCE Tip for Background
In the NMC OSCE:
- Keep information relevant as per scenario details
- Focus on patient safety
- Mention abnormal findings clearly
A – Assessment
The Assessment section explains your clinical findings and professional evaluation of the patient’s condition.
This is where nurses demonstrate clinical judgment.
What to Include in Assessment
Assessment should include:
- Information from the latest observation and compare with initial observations and all the details.
- Any other charts information (MUST, 6-CIT etc. if applicable)
- Patient pain status with pain score and medication if you administered for pain during implementation
- Details of medications administered during the implementation station.
- Health education provided
- Any referral given
You should explain what you believe is happening clinically.
Example of Assessment
In the initial assessment, his pain score was 4, respiratory rate 18, oxygen saturation 98, blood pressure 130/90, pulse: 74, and temperature: 37. 8. All observations were within the normal range, and the NEWS score was zero. Monitoring frequency: 12th hourly. Today, after surgery, I was monitoring him every 15 minutes for the first hour and every 30 minutes in the second hour. Then every hour for 4 hours after that, as per NEWS 2 policy. As per his latest assessment, his oxygen saturation was 96%, and pulse was normal, which is 84, whereas temperature was 38.4, respirations were 22 breaths per minute and blood pressure was 108/59. NEWS score 4. Comparing with initial assessment temperature and respiratory rate are elevated whereas blood pressure went lower. Mr John has reported pain, and codeine was administered from the as required. Pain reduced, but he still has nausea & tiredness. The surgical wound has beenassessed for any redness, bleeding or other abnormalities. I have also explained to him, therelaxation techniques and the importance of protein rich diet in wound healing and infectionprevention. This provides objective clinical evidence.
Why Assessment Is Critical
The Assessment section:
- Demonstrates clinical reasoning and monitoring required for patient
- Supports referral decisions
- Helps identify deterioration
- Improves patient safety
Strong assessment skills are essential in nursing because they allow early detection of serious conditions.
Objective vs Subjective Information
Objective Data
These are measurable findings:
- Blood pressure
- Heart rate
- Oxygen saturation
- Blood glucose
- Temperature
Subjective Data
These include patient-reported symptoms:
- Pain
- Dizziness
- Breathlessness
- Nausea
Effective SBAR assessment combines both.
Common Assessment Mistakes
Frequent errors include:
- Missing vital signs
- Forgetting NEWS2 and monitoring
- Missing to mention administered medications
- Unclear communication
OSCE Tip for Assessment
During the NMC OSCE:
- Include abnormal observations
- Mention NEWS2 score and monitoring
- Prioritise deterioration signs
- Speak confidently
R – Recommendation
The Recommendation section explains what action is needed next.
This is where you clearly state:
- What you need
- What you recommend
- What level of urgency exists
Many nurses feel uncomfortable making recommendations, especially when speaking to senior clinicians.

What to Include in Recommendation
Recommendations may involve, as per the handing over professional:
If handover to Dietitian, Recommendations can be:
1. Summarise the patient’s condition and request for a dietary plan
2. Recommend a reduced salt diet if the patient is on antihypertensive medication.
3. Review the MUST score to assess the patient’s nutritional risk.
4. Advise eliminating midnight snacks if the patient’s fasting blood sugar levels are elevated.
5. Emphasize the patient’s food allergies, if any.
If handover to Tissue viability nurse, Recommendations can be:
Review the wound and provide further management
1. Wound Dressing: Apply appropriate dressing and consider special dressings if required.
2. Swab Collection: Collect a wound swab for microbiological analysis to identify potential infection.
3. Debridement: Consider debridement if necrotic tissue is present.
4. Patient Education: Educate the patient and caregivers on proper wound care and signs of infection.
5. Ensure the nurse is aware of any allergies, such as latex or Elastoplast, if applicable.
If handover to Doctor Recommendations can be:
Focus on the reason for handover when giving recommendation to the doctor.
1. Patient Review
2. Vital Signs: Review vital signs.
3. Medications: Recommend any additional or alternative medications based on the patient’s concerns.
4. Further Referrals: Consider further referrals if necessary.
5. If patient has wound, then review the wound.

Why Recommendation Matters
A strong Recommendation section:
- Promotes action required
- Clarifies urgency
- Encourages teamwork
- Supports patient safety
Being Assertive Professionally
Effective recommendations should be:
- Clear
- Respectful
- Direct
- Evidence-based
You are advocating for patient safety and recommending for appropriate care.
Common Recommendation Mistakes
Errors include:
- Ending without clear action
- Failing to escalate urgency
- Avoiding recommendations completely
OSCE Tip for Recommendation
In the NMC OSCE:
- Be confident
- State urgency clearly
- Advocate for safety
- Recommend appropriate referrals

Benefits of Using SBAR in Healthcare
Using SBAR nursing communication offers multiple benefits.
Improved Patient Safety
Structured communication reduces missing information and supports early intervention.
Better Teamwork
Healthcare professionals communicate more effectively when information is organised consistently.
Faster Clinical Decisions
Clinicians receive the information needed quickly.
Reduced Communication Errors
Important details are less likely to be forgotten.
Better OSCE Performance
Students using SBAR often communicate more professionally and confidently during assessments.
How to Improve
- Practise SBAR handover
- Use simulation scenarios
- Record yourself speaking
- Focus on concise delivery
How to Practise SBAR for the NMC OSCE
Effective practice improves confidence significantly.
Step 1: Learn the Framework
Remember:
- Situation
- Background
- Assessment
- Recommendation
Step 2: Use Real Clinical Scenarios
Practise with:
- Different scenarios
- Different professionals’ handover
Step 3: Time Yourself
Good SBAR communication is concise.
Aim for:
- 2-3 minutes preparation time
- 5 minute- Clear handover
- Include Relevant details only
Step 4: Practise Speaking Aloud
Communication confidence improves through verbal repetition.
Key Tips for Effective SBAR Communication
Be Concise
Avoid unnecessary detail.
Prioritise Patient Safety
Focus on deterioration and urgent concerns.
Stay Organised
Follow the SBAR structure consistently.
Speak Professionally
Maintain calm, respectful communication.
Conclusion
SBAR communication is one of the most important professional communication tools in nursing. By using the four key components – Situation, Background, Assessment, and Recommendation – nurses can communicate patient concerns clearly, safely, and effectively.
Consistent practice, clinical understanding, and structured delivery are the keys to becoming confident with SBAR handover.

Frequently Asked Questions (FAQs)
What does SBAR stand for in nursing?
[SBAR] stands for Situation, Background, Assessment, and Recommendation. It is a structured communication framework used in healthcare to improve patient safety and communication clarity.
What information from the assessment station should be included during SBAR handover?
Under the ‘Background’ heading, include the following information from the assessment scenario:
1. Background of the current condition
2. Medical history
3. Regular medications
4. Relevant social history
5. Allergies and their reactions
What do we say under ‘Reason for Admission’ in the community scenario during evaluation? Top of Form
Mention the summary of the patient’s present condition/relevant diagnosis and the reason for visiting the patient. Bottom of Form
In the evaluation station, do we get time to write down the points before giving the handover?
Total time for evaluation is 8 minutes, so can take 2-3 minutes to prepare the short notes and in the
remaining time you verbally handover to the assessor (playing the role of a nurse/doctor/ dietician etc)
In the evaluation station, we’re required to verbalize both the initial observations and the current observations. How do we gather these two sets of observations?
In the ‘Assessment’ section, verbalise and compare the initial vital signs (along with any relevant scores such as NEWS, GCS, 6CIT, or MUST, depending on the scenario) obtained during the assessment station with the current observations provided in the evaluation scenario. Also, include the planned frequency of monitoring.